 |
Analytical Control
Systems, Inc Analytical Control Systems, Inc. |
|
|
317-841-0458
317-841-3186
Analytical Control Systems, Inc.
|
Using thromboplastins to monitoring oral anticoagulant therapy and their sensitivities to factors II, V, VII, & X Improved Prothrombin Time Reagent for Use in Oral Anticoagulant Therapy By R. Speck, July 1995 Abstract: A new thromboplastin Ultra 1 was compared with Human recombinant thromboplastin and rabbit brain thromboplastin with respect to their sensitivity to factors VII, V, X and II. It was shown that Ultra 1 is more sensitive to factors V, X and II than are the other two thromboplastins. In addition, it is totally insensitive to factor VII, which eliminates the masking effect of factor VII. This expedites the identification of patients who are stabilized on oral anticoagulant therapy.
Introduction: Hemostasis is the result of a complex series of forces. The forces which tend to cause clots to form are balanced by those forces which tend to prevent clots to form and to dissolve clots. When any of these forces gain an upper hand, the system is out of balance. When there is an inclination for thrombosis to occur, steps must be taken to reduce the risk of thrombosis. One method of treatment is the use of oral anticoagulant therapy (OAT). Vitamin K is needed for the production of the normal active K-factors. OAT drugs have molecular structures similar to vitamin K. Under the influence of the OAT drugs the protein structure is altered so that the resulting proteins cannot react with calcium ions which are required for activity of the K-factors. The K-factors are: 1)Factor VII, 2)Protein C, 3)Protein S, 4)Factor IX, 5)Factor X, 6)Factor II
See Table 1. Molecular weights, plasma concentration and half-lives of K Factors.
The level of each of the K-factors begin to decrease during OAT due to interference with their production. Each K-factor falls at a different rate. This is directly related to their in vivo half-life1,2,3,4,5. Since factor VII and protein C have very short half-lives, their concentrations decrease first and very rapidly. The order in which the other K-factors decrease is protein S, factor IX, factor X, and factor II.
The one-stage prothrombin time test has been used traditionally to monitor OAT. Commercial tissue thromboplastins from various sources are used in the prothrombin time test. Some of these are rabbit brain, beef brain, human brain, human placenta, rabbit lung, and recently, recombinant human tissue thromboplastin. The prothrombin time does not measure factor IX, protein C or protein S. Deykin6 has shown that in the early OAT the prolongation of the prothrombin time is chiefly due to the decrease in factor VII. Green and Ts'ao7 consider it doubtful that factor VII plays a major role in primary hemostasis. They base their conviction on their own research and review of the literature. Factor VII depression serves mainly to mask the concentrations of the important factors of oral anticoagulation, factors X and II. A new thromboplastin which contains no tissue factor, and therefore does not measure factor VII has recently been introduced. This thromboplastin has been designed specifically for use in OAT and consists of purified enzymes and a complex mixture of lipids which fully activate factors V and X. Factor VII is no longer an interference and changes in the prothrombin time are due only in the change in levels of factors X and II. This study compares the sensitivity of a recombinant thromboplastin (Innovin™) a rabbit brain thromboplastin (Thromboplastin C™) and a thromboplastin without tissue factor (Ultra-1™) for factors V, VII, X, and II.
Materials
Methods
Preparation of Platelet poor plasma, PPP. Draw venous blood without hemostasis from normal donor using Vacutainer No. 6415. Centrifuge at 1,000 rcf for 10 minutes. Transfer supernatant plasma with plastic Pasteur pipette to 10 x 75 polypropylene test tube. Pool three normal donor plasmas.
Outline of one-stage prothrombin time procedure.
Determining thromboplastin sensitivity for Factor V
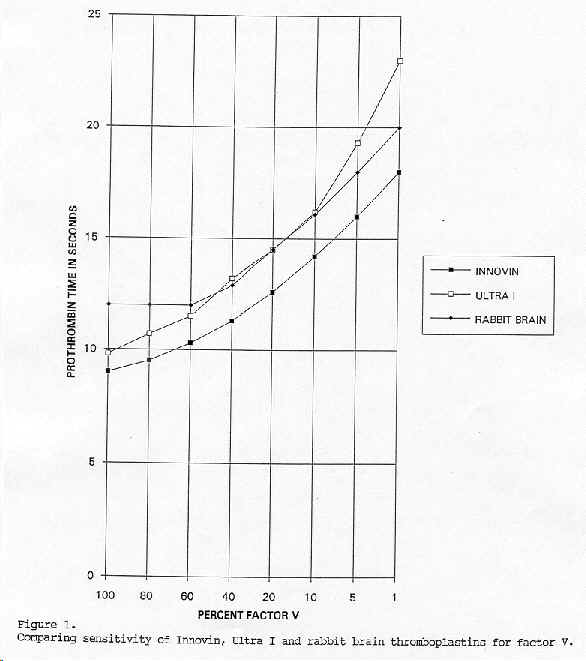
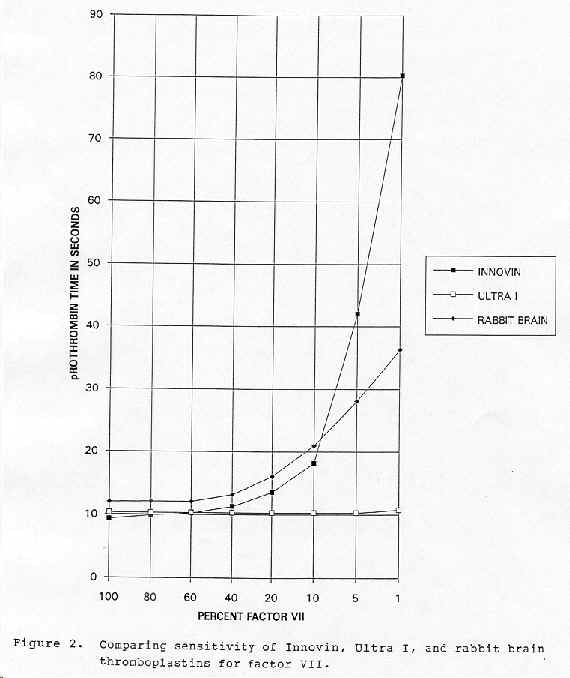
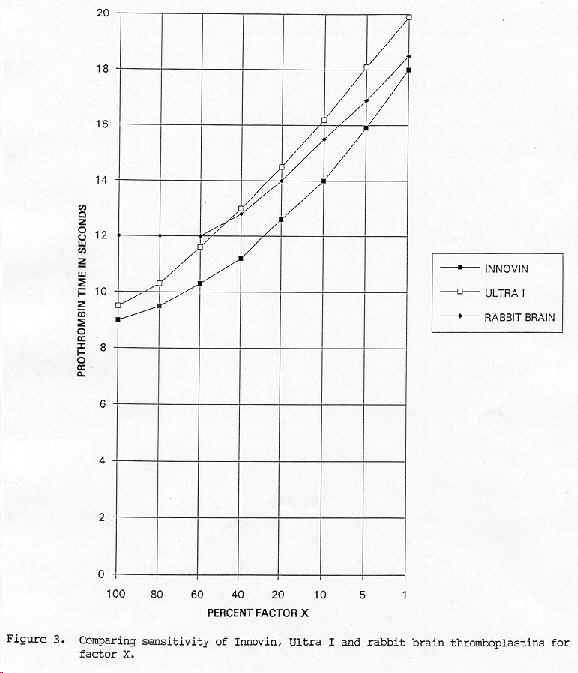
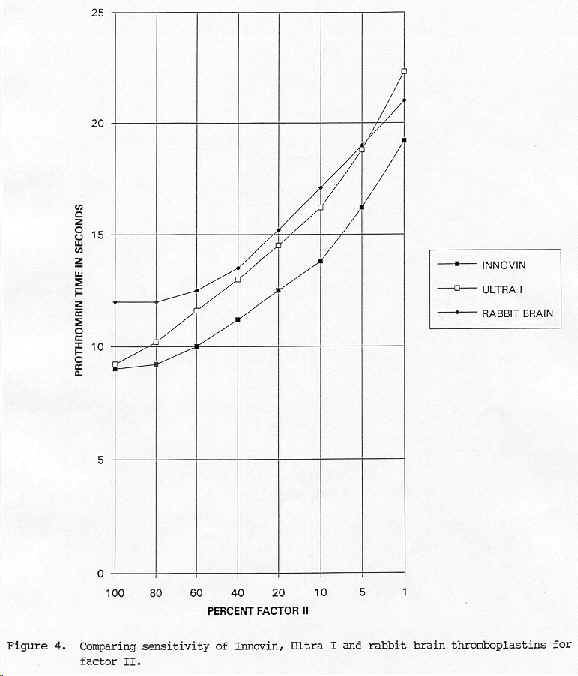
Results: Figure 1. Comparing sensitivity of Innovin, Ultra 1, and rabbit brain thromboplastins for factor V. The graph shows that on the basis of the slopes that Ultra 1 has a greater sensitivity for change in factor V levels than do the other thromboplastins. lnnovin is slightly more sensitive than the rabbit brain thromboplastin for changes in factor V. Figure 2. Comparing sensitivity of lnnovin, Ultra 1, and rabbit brain thromboplastin for factor VII. The graph shows that on the basis of the slopes that lnnovin has a very great sensitivity to change in factor VII. Rabbit brain thromboplastin is moderately affected by change in factor VII. Ultra I is not affected at all by change in factor VII. Figure 3. Comparing sensitivity of lnnovin, Ultra 1, and rabbit brain thromboplastins for factor X. The graph shows that Ultra I is more sensitive to change in factor X than either of the other two thromboplastins. lnnovin shows a slightly greater sensitivity to change in factor X than does the rabbit brain thromboplastin. Figure 4. Comparing sensitivity of lnnovin, Ultra 1, and rabbit brain thromboplastin for factor II. The graph shows that Ultra 1 is more sensitive to change in factor II than are either of the other two thromboplastins. lnnovin appears to be more sensitive than the rabbit brain thromboplastin in the high ranges but less sensitive than the rabbit brain thromboplastin in the therapeutic range.
Discussion: It is well documented that commercial thromboplastins from different sources and methods of preparation vary to a great extent in their responsiveness to OAT. Consequently, prothrombin test results from different laboratories are not intercomparable for patients on OAT. In order to correct for this difference in slope of various commercial thromboplastins, the World Health Organization (WHO) established an international committee whose object was to develop a system which would make possible the comparison of prothrombin time results from different laboratories.. They finally approved a system, called the International Normalized Ratio (INR) system8. The principle involves comparing the test thromboplastin with the WHO certified thromboplastin for which an international sensitivity index (ISI) had been determined. Twenty normal patients and 60 OAT stabilized patients had prothrombin time determinations performed using both the WHO certified thromboplastin and the test thromboplastin. The logarithms of the prothrombin times were determined. An orthogonal regression was performed to find the slope. It must be noted that the INR system only applies to stabilized patients. The definition of a stabilized patient is in question. This is important since in the OAT induction period protein C and factor VII levels fall rapidly to a very low level within 24 hours. This is a result of their short half-lives. At this stage there is an added risk for thrombus formation because of the lowered protein C level. Heparin therapy must continue until factors X and II levels are decreased sufficiently to protect the patient from further risk of thrombosis. Only then is it safe to stop the heparin therapy. At the present time, one must guess when this stabilized state occurs. Because of the masking effect of factor VII when using tissue thromboplastin in the prothrombin test, it is not possible to know with any certainty when the patient if stabilized. On the other hand, when using Ultra 1 thromboplastin, factor VII is not an interference. The prothrombin times with this thromboplastin is directly related to the levels of factors X and II. This makes it possible to ascertain when a patient is stabilized.
Summary: The use of the INR system in OAT has improved patient care to a large extent. Still, there are limitations. Some of these are variations in sensitivity of commercial thromboplastins to K-factors, masking by factor VII and inability to known when a patient is stabilized. The introduction of Ultra 1 can remove these limitations. This thromboplastin has greater sensitivity for factors X and II, is not affected by factor VII and identifies when the patient is stabilized with great precision.
References:
| |||||||||||||||||||||||||||||||||