 |
Analytical Control
Systems, Inc Analytical Control Systems, Inc. |
|
|
317-841-0458
317-841-3186
Analytical Control Systems, Inc.
|
Platelet Aggregation SPAT™ An Explanation A platelet aggregation test is available on a slide. This Slide Platelet Aggregation Test™ offers an alternative (or augmentation) to expensive platelet aggregometer testing and/or tricky bleeding time tests. For many years there was no real alternative to the bleeding time test and platelet aggregometry. The invention of ACS's new, patented aggregation reagent changes all that. SPAT™ is potent enough to allow it to be performed on a slide, and it is useful as a uniquely sensitive screen for many different types of platelet dysfunction. The bleeding time test was originally the most popular alternative to aggregometry. Its two basic benefits were its relatively low cost and the speed at which it could be performed. However, these benefits were balanced by many in-vivo problems. Bleeding time is not a specific in-vivo indicator of platelet function7. It is effected by a wide range of conditions that include such sweeping categories as anxiety, age, ethnicity and gender5. There is even indication that the bleeding time test has no proven value as a preoperative evaluation for patients receiving aspirin or NSAIDs, patients with liver disease, patients for coronary bypass, or even patients for general surgery6. In addition, it has not been proven that it can predict bleeding in patients with myeloproliferative disease or newborn infants given NSAIDs6. SPAT™, however, can offer both the speed of a useful presurgical screening test and a low cost test that does not require the use of an aggregometer. The study below indicates the performance of the SPAT™ test when run side-by-side with the bleeding time test.
Clinical Data Normal Ranges for PT, APTT, Bleeding Time and SPAT™ Dr. Melvin of Sparrow Hospital performed a study on surgical outpatients to determine the normal ranges on 4 tests and to examine scientifically the performance characteristics of SPAT™ as a preoperative screen.
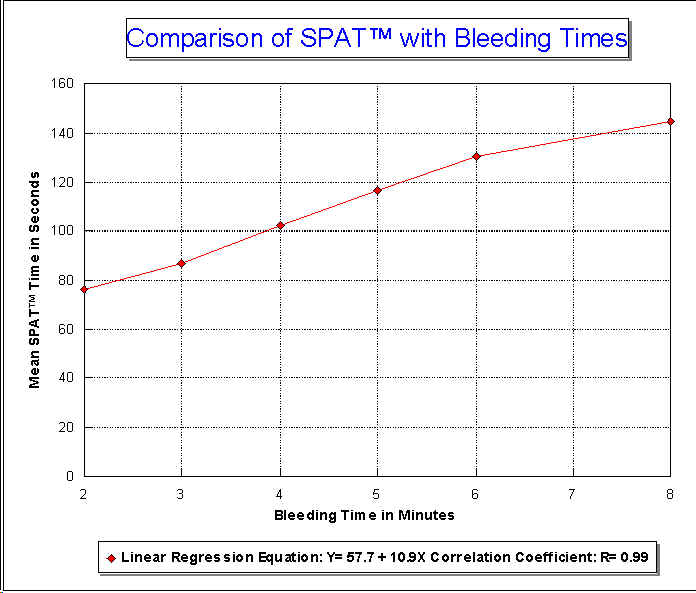
A study of one hundred consecutive surgical outpatients between the ages of 2 and 89 was performed at Sparrow Hospital, Michigan by J. R. Melvin, Jr., Ph.D., Director of Hemostasis, which compared one stage Prothrombin Time, APTT, Bleeding Time and SPAT™ in order to set normal ranges for SPAT™ and to relate the clinical data revealed about patient's platelets from bleeding time tests and SPAT™. Normal ranges were set as follows:Prothrombin time: 10-12 seconds APTT: 22-34 seconds Bleeding time: 2-8 minutes Slide Platelet Aggregation Test: Less than three minutes Of one hundred patients, one had an abnormal APTT and bleeding time, and a normal SPAT™. Another patient had a normal APTT, bleeding time and an abnormal SPAT™. This patient was taking aspirin or an aspirin containing compound. A third patient had a normal APTT, abnormal bleeding time and abnormal SPAT™. His case was confirmed as type 1 von Willebrand disease. The correlation between normal range bleeding time results and mean Slide Platelet Aggregation Test times is very high. The following linear regression equation and graph shows a high correlation coefficient at R = 0.99.
Bleeding Time and SPAT™ Comparison of the SPAT™ & Bleeding Times SPAT™ results correlate well with the bleeding time test.
Figure 4. Comparison of bleeding times in the normal range (2-8 minutes) and mean Slide Platelet Aggregation Test results on 93 patients ranging in ages from 2 to 89 years old. Linear regression equation: Y = 57.7 + 10.9X. Correlation Coefficient: R= 0.99
Table 5. Data Points for Figure 1.
Performance of SPAT™ vs. PAF-16, Collagen, ADP, Epinephrine, Ristocetin and Arachidonic Acid Comparison of Various Platelet Aggregating Reagents with ACS's SPAT™ Reagent Using a Slide Platelet Aggregation Procedure In the slide procedure, SPAT™ produces larger clumps than all but PAF-16. Only the powerful aggregator PAF-16 and ADP (which circumvents the natural release of ADP) had shorter normal times for this patient.
O ne of the chief benefits of SPAT™ is its ability to produce aggregates capable of being visually detected. Shown below is SPAT™'s performance compared to other aggregating reagents.
Table 6. SPAT™ and most of the common aggregating reagents were compared for aggregation strength and time using a slide procedure. SPAT™ ranks as one of the strongest aggregators with a comparably short aggregation time for normal patients.
Platelet Count and SPAT™ Effect of Platelet Count on SPAT™ SPAT™ results are within the normal limits and 3+ aggregation down to a platelet count of approximately 32,000 mm3.
W hen performing the SPAT™ procedure it is important to obtain a sample rich in platelets. Shown below are the results from a study run on a sample from the same normal patient where the percent of platelet rich plasma was gradually reduced. Although the study showed that SPAT™ results remained in the normal range until 6.25% where there was no longer enough platelet count to support aggregation, the best accuracy was achieved with the optimal level of platelets (255,000 platelets per mm3). Halving the number of platelets resulted in an increase of 50 seconds. However, the diagnosis of this patient did not change until an extremely low level of platelets was reached. Such a count (15,900 platelets per mm3) could not support any kind of accurate platelet testing. However, it is because the reagent is not extremely sensitive to the platelet count that it is so useful as a manual slide test.
Table 7. SPAT™ is reliable with plasma with a platelet count as low as 32,000/mm3 while an optical aggregometer is unreliable below 100,000/mm3.
Temperature and SPAT™ Effect of Temperature on SPAT™ Varying the temperature from 20o C to 37o C has no effect on the results obtained with the SPAT™ procedure.
A nother indication that SPAT™ can be accurately performed on a manual slide procedure is the range of temperatures at which it can be run without adversely effecting the results. In addition, with SPAT™'s 30 day reconstituted, refrigerated stability, a laboratorian need not worry about taking the time necessary to insure that the reagent reaches 32o C. prior to testing.
Table 8. Although the reagent has a fairly wide band of temperatures at which it is useful, it is important to warm the reagent to room temperature to prevent artificially prolonged times.
Heparin and SPAT™ Effect of Heparin on SPAT™ Heparin dosages up to 4.0 units per ml. do not effect SPAT™ results.
A study of the effect of heparin on SPAT™ results shows that the procedure can be safely run without the addition of heparinase.
Table 9. There is little effect on SPAT™ by heparin and heparinase.
SPAT™ and Clinical Conditions SPAT™ as a Screening Test SPAT™ shows great sensitivity to many conditions that put the patient at risk of bleeding during surgical procedures.
A dditional ongoing studies have indicated that the Slide Platelet Aggregation Test is very sensitive and will demonstrate the impact by many substances on the aggregation of platelets3. One such study involving well known platelet aggregation inhibitors is presented on the next page. Unlike many of the other aggregating compounds, SPAT™ results are significantly changed by the addition of all three inhibitors (Cyclic AMP, PGI2 and EDTA). The fact that no aggregation is possible in the presence of EDTA indicates that SPAT™ does not circumvent the natural need for calcium ions to be present for aggregation to occur.
SPAT™ with Cyclic AMP, PGI2, and EDTA Effect of Platelet Aggregation Inhibitors on Common Platelet Aggregating Compounds and SPAT™ on the Slide Platelet Aggregation Procedure SPAT™ shows strong sensitivity to known aggregation inhibitors.
Table 10. Some reagents show no sensitivity to known platelet aggregation inhibitors. SPAT™ times, however, are significantly lengthened by Cyclic AMP and PGI2. As predicted by the need for some calcium atoms to be present for aggregation to occur, SPAT™ and all the other reagents tested produced no aggregation with EDTA present.
SPAT™ with Aspirin, Dipyridimol, Coumadin, Type I von Willebrand, Bernard Soulier Defect, Storage Pool Disease, and DIC SPAT™ Values from Patients with Clinical Conditions SPAT™ is very sensitive to many of the conditions which would put a patient at risk for bleeding.
B lind studies have indicated that patented SPAT™ is very responsive to therapies and disease states that would put a patient at risk for bleeding. The conditions for which SPAT™ displayed abnormally lengthened times included aspirin therapy, dipyridimol therapy, coumadin therapy, type I von Willebrand disease, Bernard Soulier defect, Storage pool disease and DIC. Additional studies are in progress.
Table 11. SPAT™ is sensitive to Aspirin therapy, Type I von Willebrand, Dipyridimol therapy, Bernard Soulier defect, storage pool disease, DIC, and Coumadin therapy.
Bibliography
End.
|