 |
Analytical Control
Systems, Inc Analytical Control Systems, Inc. |
|
|
317-841-0458
317-841-3186
Analytical Control Systems, Inc.
|
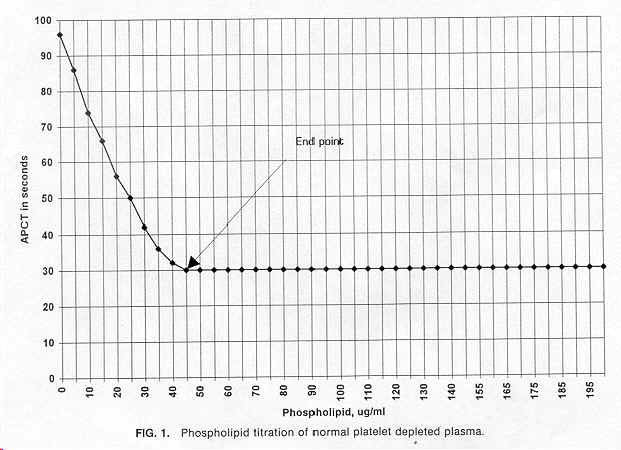
Titration of the Lupus Anticoagulant New Method for Quantifying Lupus Anticoagulant By Roy Speck. June 1996. Summary: A method is presented using a new reagent containing propyl gallate for the quantitative determination of lupus anticoagulant. The amount of an optimized phospholipid standard required by the clotting reaction was found to be 32-50 ug/ml at a 95% confidence level, with a mean of 41 ug/ml. This method eliminates the effect of heparin therapy, coumadin therapy, factor VIII inhibitor, factor IX inhibitor, and single-factor deficiencies that afflict presently used lupus anticoagulant screening and confirmatory procedures. Using this method, it should be possible to detect lupus anticoagulant in patients at a much lower level and follow the effect of therapy on lupus anticoagulant. Key Words: Lupus anticoagulant, phospholipid, activated plasma clotting time (APCT), activated partial thromboplastin time (APTT). Lupus anticoagulant (LA) is characterized as anti-phospholipid antibodies (APA) that interfere with phospholipid-dependent clotting tests. LA is associated with arterial and venous thrombosis (1-4), as well as recurrent spontaneous abortion (5,6). The screening tests for LA are not entirely satisfactory. The procedures commonly in use lack sensitivity and exhibit a substantial amount of variation. Even the most recent studies do not show any general agreement regarding an acceptable procedure for detecting LA (Table 1). Guidelines on testing for LA have been issued by the British Society for Hematology (14) and SSC Subcommittee for the Standardization for Lupus Anticoagulant (15): There should be a prolongation of phospholipid dependent clotting tests, that is, kaolin clotting time, dilute Russell viper venom time, tissue thromboplastin inhibition test, plasma recalcification clotting time, or a sensitive activated partial thromboplastin time (APTT) test. Clotting times of a mixture of test and normal plasma should be significantly longer than that of a mixture of non-LA plasma and normal plasma. There should be a correction of the prolonged test result when there is an addition of lysed, washed platelets, phospholipid liposomes containing phosphatidyiserine, or hexagonal phase phospholipids. The test results should be nonspecific for any individual clotting factor and include a positive enzyme-linked immunosorbent assay for antiphospholipid antibody. Even when the confirmatory procedures are performed on plasma samples that demonstrate prolongation of the test results by the screening LA procedures, it is not always possible to identify an LA. At best, LA can be identified as weak, moderate, or strong. I have developed a new soluble chemical activator, propyl gallate, which rapidly activates the intrinsic pathway, as well as platelet factor 3 found in the platelet membrane. Removing the platelets by filtering plasma through a 0.22 um membrane filter and performing an activated plasma clotting time (APCT) that using this new reagent results in an increased sensitivity in detecting LA because of the low phospholipid present in the reaction. The platelet membrane microfragments in the filtrate supply the phospholipid used in the clotting reaction. I have also developed a purified optimized phospholipid that can be added in increasing known amounts to this reagent. By performing the APCT test using this reagent with different phospholipid content, the amount of LA present in the patient's plasma can be quantified. This study demonstrates the advantages offered by this new technique. The study plan is (a) determine normal phospholipid requirements for coagulation and (b) compare APCT, APTT, and phospholipid content while using normal and various abnormal plasmas.
Materials and methods: Materials
Methods:
Preparation of platelet-depleted plasma A clean venipuncture was performed without hemostasis using Vacutainer 6415 containing buffered 0.109 M sodium citrate. Samples were mixed immediately and centrifuged for 10 min at 2,000 RCF. The platelet poor plasma (PPP) was transferred to a plastic test tube with a plastic Pasteur pipette. The PPP was filtered through 0.22-um membrane filter into plastic test tube. The platelet-depleted plasma (PDP) samples were stored at room temperature for no longer than 2 hours. Hemolyzed samples were discarded.
Determination of activated plasma clotting time APCT reagent (100 ul) and PPP (100 ul) were added to a reaction cuvette and mixed. After incubation at 37�C for exactly 3 min, 100 ul 0.02 m CaCl2, which had been prewarmed at 37�C for at least 3 min, was added and the clotting time determined.
Determination phospholipid requirements for normal plasma PDP samples were prepared from 40 adult donors who were taking no medication. The phospholipid requirement for each sample was determined and the 95% confidence limit was calculated. The procedure outline was as follows:
Results: Phospholipid required for clotting reaction was determined (n = 40, mean = 41 ug/ml phospholipid, and 95% confidence limit = 32-50 ug/ml phospholipid), and APCT, APTT, and LA phospholipid assay results for normal and abnormal plasmas were contrasted (Table 2).
Discussion: LA neutralizes the phospholipid in the reaction mixture of in vitro phospholipid-dependent clotting tests. When the phospholipid content falls below that amount needed to support the clotting reaction,the test results become prolonged. However, a number of conditions can also prolong the test result. Among these are
Because of these other possibilities for prolonged test results, additional procedures are necessary so that these other possibilities may be eliminated and the presence of LA may be confirmed. Mixing studies and agarose gel electrophoresis are used to identify inhibitors. Confirmatory procedures using test systems with decreased phospholipids are tissue thromboplastin inhibition, dilute Russell viper venom test, and dilute phospholipid APTT test. Confirmatory procedures using test systems with increased phospholipids are platelet neutralization procedure, high phospholipid APTT, rabbit brain neutralization, phosphatidyiserineliposome APTT, and hexagonal phospholipid neutralization. Even when these other procedures are performed, the only thing that can be determined is whether the LA is weak or strong. On the other hand, by determining the quantity of phospholipid needed to satisfy the requirements for the clotting reaction, these other interferences are eliminated. In fact, the results are essentially a quantitative measurement of the LA present in the patient's plasma. It may become necessary to redefine LA to include that antiphospholipid antibody which neutralizes the phospholipid that exceeds that which is required for the clotting reaction. With this LA-quantifying procedure, the true incidence of LA and the level of LA that is clinically significant can be determined. In addition, it is possible to follow the effect of therapy on the level of LA and perhaps assist in development of new pharmaceuticals for their effect on LA.
References:
APA, anti-phospholipid antibodies; APTT, activated partial thromboplastin time; DRVVT, dilute Russel viper venom time; KCT, kaolin clotting time; LA, lupus anticoagulant; PNP, platelet neutralization procedure; and TTIT, tissue thromboplastin inhibition test
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||